
The Liminal Trap
Why insight alone doesn’t move the nervous system


I recently came across a post by a psychedelic plant-medicine facilitator describing what’s sometimes called the liminal trap: a form of internal stuckness that can be difficult to recognize but is deeply felt by an individual.
In healthy transitions, liminal states are temporary. They resolve as the nervous system adapts and movement resumes. In trauma, however, these states often become chronic, not just psychological and rooted in biology.
Trauma and the Nervous System: Why the Trap Forms
Trauma doesn’t just live in memory—it changes the body at a biological level. When something overwhelming happens, especially when there’s no way out, the nervous system adapts to survive. The brain’s threat circuits become more reactive, stress hormones stay elevated, and the systems meant to calm and regulate the body lose influence. Memories of the event are stored in a raw, sensory way, so the body reacts as if the danger is still happening. Over time, the nervous system learns a hard rule: movement, change, or action leads to danger. What looks like being stuck isn’t failure; it’s a body that learned stillness was the safest option.1
This is why people with trauma often say things like:
“I know what I should do, but I can’t do it.”
“I feel frozen.”
“I’m exhausted from thinking, but nothing changes.”
“I don’t feel like myself anymore, but I don’t know who I am now.”
To be more specific about how the body changes, check this chart out:
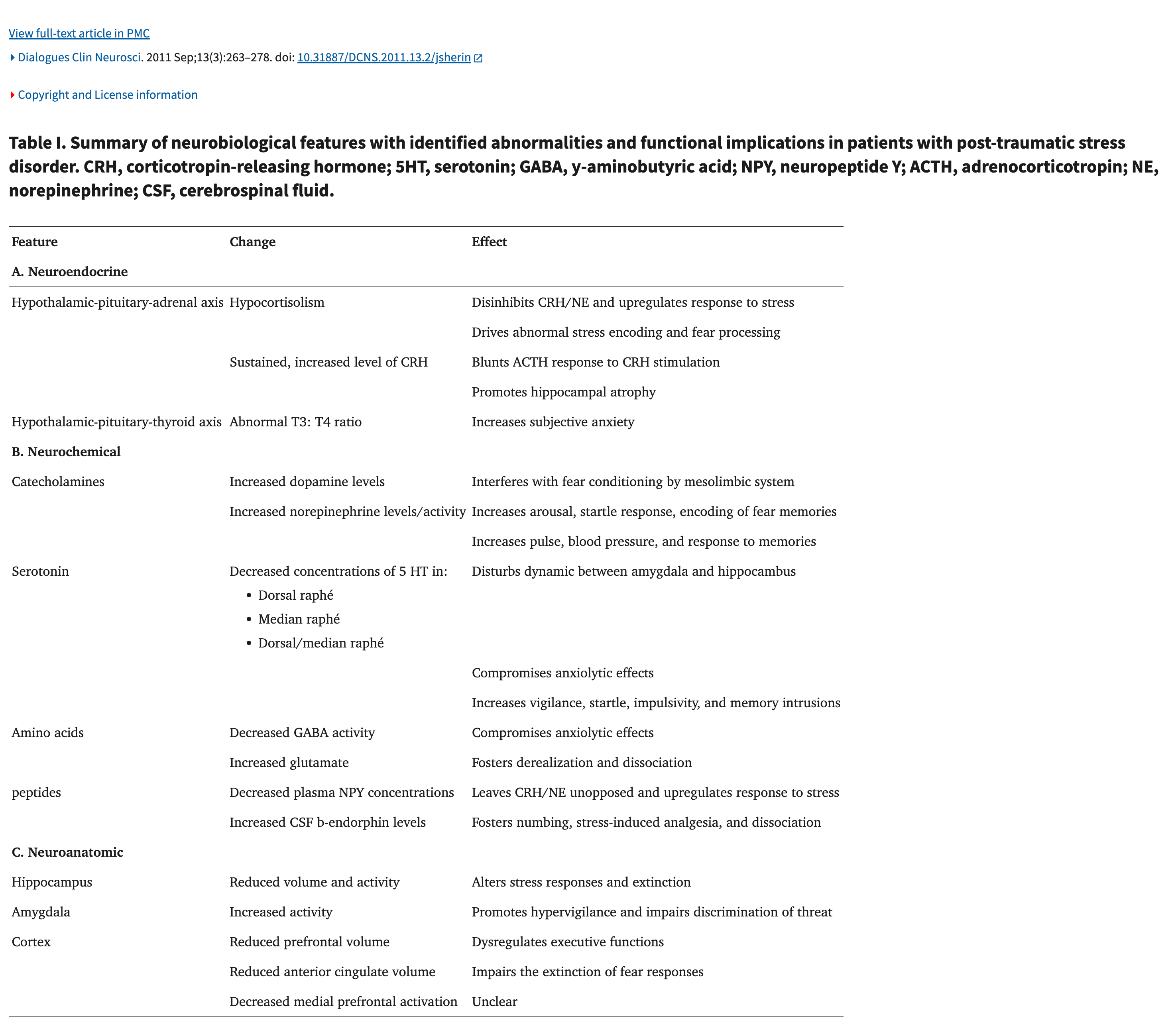
The chart shows that trauma leads to concrete biological changes in the brain and nervous system. The systems that manage stress hormones become dysregulated, so the body has trouble shutting off a stress response once it starts. Neurochemicals that drive alertness and threat detection become overactive, while those responsible for calming, inhibition, and emotional regulation are reduced. At the same time, brain regions involved in detecting danger become more reactive, and regions responsible for regulation, context, and control lose influence. These shifts create a nervous system that is biologically primed to expect threat, react quickly, and avoid movement or engagement, because stillness once increased the chance of survival.
Why Naming the Liminal Trap Is Only the Beginning
Identifying that you’re stuck in a liminal trap creates awareness, but awareness alone does not reverse the biological adaptations that trauma creates. Trauma reshapes stress systems, hormones, sleep regulation, and nutrient-dependent processes in the body. Without addressing these physiological foundations alongside psychological work, insight can clarify why someone is stuck without giving the nervous system the conditions it needs to change. What follows are key biological domains that research shows must be addressed for recovery to move beyond understanding into actual regulation and movement.
Hormones & Stress Biology
Chronic stress and trauma disrupt the hypothalamic-pituitary-adrenal (HPA) axis, the system responsible for regulating cortisol and other stress hormones. In trauma-exposed individuals, cortisol responses can become blunted or mistimed, while upstream stress signals remain elevated, leaving the body in a prolonged state of threat readiness. This dysregulation is influenced not only by psychological stress but also by sleep, nutrition, and overall physiological load, meaning therapy alone cannot fully normalize stress signaling without biological support.2
Vitamin D & the Stress Response
Clinical research has found that individuals with PTSD frequently have significantly lower vitamin D levels than healthy controls. These deficiencies are associated with abnormal regulation of HPA-axis hormones such as corticotropin-releasing hormone (CRH) and adrenocorticotropic hormone (ACTH), as well as altered cortisol levels. Low vitamin D appears to impair the body’s ability to regulate stress responses effectively, suggesting that deficiency can biologically reinforce ongoing dysregulation even when psychological insight is present.3
Vitamin C & Cortisol Regulation
Vitamin C plays a direct role in adrenal function and cortisol metabolism. Randomized clinical studies show that supplementation around 1,000 mg per day can reduce elevated cortisol and DHEA-S levels in individuals under chronic stress. Additional research demonstrates that vitamin C administered before acute stress accelerates the return of cortisol to baseline afterward, indicating improved physiological recovery rather than mere subjective calm. These findings support the idea that adequate vitamin C helps the stress system complete its cycle instead of remaining stuck in activation.4
Nutrition & Mental Health
Broad nutritional research shows that adequate intake of key micro- and macronutrients—including fatty acids, magnesium, and vitamins—directly affects brain chemistry, hormone signaling, inflammation, and stress tolerance. Nutrient deficiencies are associated with impaired emotional regulation, increased anxiety, and reduced resilience, all of which can biologically limit recovery from trauma even when psychological insight is strong.5
Sleep & Recovery
Across multiple studies, inadequate sleep is associated with higher rates of anxiety, depression, irritability, and impaired coping, along with increased stress sensitivity and reduced resilience. Sleep loss disrupts hormonal balance, immune function, and cognitive control, making it harder for the brain and body to recover from daily stressors. Importantly, the findings suggest that poor sleep doesn’t just worsen existing mental health issues—it can actively contribute to their development and persistence, reinforcing cycles of dysregulation rather than allowing recovery.6
What Actually Helps the Nervous System Shift
Once the biological foundations of stress and recovery are supported, the next step is giving the nervous system new experiences that contradict what trauma taught it. This is where therapy and embodied regulation practices are important.
EMDR
EMDR, or Eye Movement Desensitization and Reprocessing, is a trauma therapy that works with how the nervous system actually stores threat. Instead of relying on insight or retelling the story over and over, EMDR helps the brain reprocess memories that got stuck during overwhelming experiences.7 While briefly bringing a traumatic memory to mind, the person engages in bilateral stimulation, often through guided eye movements or tapping. This allows the nervous system to recognize that the event is over. The memory doesn’t disappear, but it loses its intensity. What once triggered fear, shutdown, or panic becomes something that happened in the past, not something the body is still bracing for.

Breathwork and Yogic Breathing and Movement
Having had a yoga background in education, I have known for many years that yoga and breathwork reduce stress. Breathwork and other controlled breathing practices directly influence the autonomic nervous system, lowering physiological arousal and improving emotional regulation.8
Activities
Regular movement-based activities—whether structured exercise or experiential activities like hiking, surfing, or golf—combine rhythm, focus, sensory input, and mild challenge, all of which help the nervous system relearn safety in motion. Research consistently shows that these approaches reduce stress hormones, improve mood, and increase resilience not by insight alone, but by repeated, embodied experiences of regulation and mastery.9
The Use of Psychedelic Therapy in Trauma
It’s impossible to talk honestly about trauma recovery without acknowledging the growing body of research on psychedelic-assisted therapy. Substances such as psilocybin10, ayahuasca11, and iboga-derived compounds12 have shown potential to reduce trauma-related symptoms, depression, addiction, and emotional rigidity—but not because they “fix” trauma on their own. What these compounds appear to do is temporarily loosen the nervous system’s grip on entrenched patterns of fear, avoidance, and shutdown, creating a window in which new learning becomes possible. Note that the ibogaine study does have funding provided by the non-profit The Mission Within, and there are also some conflicts of interest within the researcher list.
Research suggests that psychedelics increase neuroplasticity, reduce rigid threat responses, and allow traumatic material to surface without the same level of defensive overwhelm. However, outcomes depend heavily on context. Without preparation, therapeutic support, and post-experience integration, these experiences can be destabilizing or short-lived. Psychedelics are not replacements for therapy; they function best as amplifiers of therapeutic work already in motion.
One must also consider that using plant medicine is not simply popping a pill, there is ceremonial ritual involved in the process. For example, the research emphasizes the importance of studying and respecting the full ceremonial framework rather than isolating the compound alone. With careful, well-regulated research that honors these components, ayahuasca may emerge as a holistic therapeutic approach for certain psychological disorders rather than a conventional pharmaceutical intervention.13 This could be applied to any of the plant medicines and their ritual use.
For trauma specifically, the most effective use appears to involve pairing psychedelic experiences with structured modalities such as EMDR and breathwork. EMDR helps reprocess traumatic material that becomes accessible during or after psychedelic experiences, while breathwork supports nervous system regulation before, during, and after these altered states. Together, these approaches help translate insight into integration, allowing the nervous system to learn safety rather than simply revisit intensity. Psychedelic therapy works not because of the substance alone, but because of the preparation, containment, and follow-through that surround it.
Moving Through and Exiting the Liminal Trap
People who actually move out of liminal trauma states don’t do it through a single insight or breakthrough; they change the conditions their nervous system is living in.
They start by prioritizing sleep, nutrition, light, movement, and reducing chronic stress, because a dysregulated system can’t integrate insight, no matter how profound it feels. The personal work exists in clear containers, such as trauma-informed therapy, structured group work, or well-designed retreat settings, because boundaries create safety, and safety allows movement. The focus remains less on the experience itself and more on integration, and that is where the real shift happens
My book and audiobook offer a broader blueprint for building resilient health—not quick fixes, but the foundations that support real, lasting change. If you’re looking for thoughtful, personalized support as you navigate this work, I also offer health consulting grounded in safety, integration, and sustainability.
Sherin, Jonathan E., and Charles B. Nemeroff. “Post-Traumatic Stress Disorder: The Neurobiological Impact of Psychological Trauma.” Dialogues in Clinical Neuroscience 13, no. 3 (September 2011): 263–278.
Sherin, Jonathan E., and Charles B. Nemeroff. “Post-Traumatic Stress Disorder: The Neurobiological Impact of Psychological Trauma.” Dialogues in Clinical Neuroscience 13, no. 3 (September 2011): 263–278.
M. H. Al-Delaimy et al., “Vitamin D Deficiency and Hypothalamic–Pituitary–Adrenal Axis Dysregulation in Post-Traumatic Stress Disorder,” Frontiers in Neuroscience 19 (2025).
H. Peters et al., “Ascorbic Acid Accelerates Cortisol Recovery After Acute Psychological Stress,” European Journal of Clinical Nutrition 70, no. 6 (2016): 675–681.
Firth, Joseph, et al. “Dietary Improvement for Symptoms of Depression and Anxiety: A Meta-Analysis of Randomized Controlled Trials.” Library of FAB Research. Accessed February 3, 2026.
Shah, Arambh Sanjay, Mitresh Raj Pant, Tulasiram Bommasamudram, Kirtana Raghurama Nayak, Spencer S. H. Roberts, Chloe Gallagher, K. Vaishali, Ben J. Edwards, David Tod, Fiddy Davis, and Samuel A. Pullinger. “Effects of Sleep Deprivation on Physical and Mental Health Outcomes: An Umbrella Review.” American Journal of Lifestyle Medicine, May 27, 2025.
Chen, Ying-Ran, Kuo-Wei Hung, Jeng-Chi Tsai, Hui-Chun Chu, Mei-Hua Chung, Shu-Ruey Chen, Yu-Ming Lee, and Feng-Yu Yang. “Efficacy of Eye-Movement Desensitization and Reprocessing for Patients with Posttraumatic Stress Disorder: A Meta-Analysis of Randomized Controlled Trials.” PLoS ONE 9, no. 8 (2014).
Brown, Richard P., and Patricia L. Gerbarg. “Sudarshan Kriya Yogic Breathing in the Treatment of Stress, Anxiety, and Depression: Part II—Clinical Applications and Guidelines.” Journal of Alternative and Complementary Medicine 11, no. 4 (2005): 711–717.
Wang, Zhi Feng, Bing Jiang, Xingtong Wang, Zhixiang Li, Dongxu Wang, Hai Hong Xue, and Dongmei Wang. “Relationship between Physical Activity and Individual Mental Health after Traumatic Events: A Systematic Review.” European Journal of Psychotraumatology 14, no. 2 (2023).
Carhart-Harris, Robin L., Matthew Bolstridge, C. M. J. Day, J. Rucker, Rosalind Watts, D. E. Erritzoe, M. Kaelen, B. Giribaldi, M. Bloomfield, S. Pilling, J. A. Rickard, B. Forbes, A. Feilding, D. Taylor, H. V. Curran, and D. J. Nutt. “Psilocybin with Psychological Support for Treatment-Resistant Depression: Six-Month Follow-Up.” Psychopharmacology 235, no. 2 (2018): 399–408.
Sheth, R., E. Parikh, K. Olayeye, and K. Pfeifer. “The Effects of Ayahuasca on Psychological Disorders: A Systematic Literature Review.” Cureus 16, no. 3 (2024): e55574.
Davis, Alan K., Lynnette A. Averill, Nathan D. Sepeda, Joseph P. Barsuglia, and Timothy Amoroso. “Psychedelic Treatment for Trauma-Related Psychological and Cognitive Impairment Among U.S. Special Operations Forces Veterans.” Chronic Stress 4 (July 8, 2020): 2470547020939564.
Sheth, R., E. Parikh, K. Olayeye, and K. Pfeifer. “The Effects of Ayahuasca on Psychological Disorders: A Systematic Literature Review.” Cureus 16, no. 3 (2024): e55574.